Spending Review 2020-2021 – Funding of homecare services
The following letter was sent to the Department of Health and Social Care before the anticipated spending review for 2020-2021. UKHCA first met with the Department’s Spending Review team in April 2019.
Formal submissions from stakeholders had not been requested prior to the announcement by HM Treasury that a spending round would cover just one year and would be published on 4 September 2019.
These extremely short timescales have been rumoured to be potential a signal of a snap general election. UKHCA believes that the issues which are outlined in our submission are important not just for the spending announcement covering 2020-21, but for preparation by the Government of the day, which will need to plan for a three- or five- year spending review in the coming year.
____________________________________________________________________________________
Dear Secretary of State,
As the Department of Health and Social Care embarks on its contribution to the next Spending Review, we are writing to you so that you are aware of the financial position of state-funded homecare and where future investment is needed.
United Kingdom Homecare Association (UKHCA) is the national professional and representative association for organisations who provide care, including nursing care, to people in their own homes.
We are a member-led professional association; our mission is to promote high quality, sustainable care services so that people can continue to live at home and in their local community. We represent over 2,000 homecare providers in the UK, including those which support people in receipt of State-funded homecare and others who purchase support from their private means.
Over 4.1 million hours of state-funded homecare are purchased each week in the UK. This enables over 850,000 people to be supported to live at home independently each year. The size of the privately purchased homecare market is not known with certainty, but may represent a further 1.75 million hours and 364,000 people.
We have set out the key factors we consider the Department of Health and Social Care and the Treasury should consider in the Spending Review in the submission which accompanies this letter. We summarise them below.
Inevitably, some of the issues we discuss are wider than those which can be addressed in a short-term spending round of just one year, but they are issues which will require urgent preparation to be done during the spending round period so that they can be acted upon before the spending round which will follow it.
1. Invest in the workforce
Our dedicated and skilled workforce are the most important part of effective social care services.
Government should:
- Ensure the fees paid by local authorities to homecare providers who deliver state-funded care are sufficient to allow attractive rates of pay which will facilitate recruitment, retention, investment in skills training and allow for differentials for those in more senior roles or with greater experience or responsibilities.
- Provide local authorities with sufficient resources so that they can pay for services at a level which ensures that providers can meet their legal and social responsibilities. We believe that, given the proportion of homecare purchased by the state, adequate funding will raise the status of the entire social care workforce, including those who support people who fund their own care.
- Produce a workforce plan that ensures there are sufficient numbers of well-trained homecare workers to meet the needs of an increasingly ageing population.
- Ensure that the UK’s post-Brexit migration policy is effective and reflects a future workforce strategy.
- Review the operation of apprenticeships, so that they are more suitable for the needs of homecare providers, including those organisations which must pay the apprenticeship levy.
2. Invest in a sustainable, vibrant and diverse market
- Plug the gap in funding homecare services across the UK to stabilise the homecare market. We estimate that is a minimum of £599 million this year at a rate which would meet the current statutory minimum wage levels, or £1.08 billion for a sector which would be able to meet the rate of the independently calculated Living Wage.
- Provide for independent oversight of commissioning of adult social care by local authorities in England, to ensure that market shaping responsibilities under the Care Act 2014 are effectively monitored and authorities are required to take corrective action where they fail to comply.
- Ensure that the commissioners of health and social care services are working to deliver services which can reduce pressures on the NHS, and recognise the unique contribution that homecare providers can make in reducing those pressures by reducing risks to market stability.
3. Take actions which reduce cost pressures on social care providers
- Change the VAT status of ‘welfare services’ from ‘exempt’ to ‘zero-rated’, to enable providers to recover their “input tax”.
- Resolve the risk of National Minimum Wage claims in relation to ‘sleep-in’ duties.
- Legislate to amend new case-law on holiday pay following the Court of Appeal ruling in Harpur Trust v Brazel & Unison.
4. Ensure the public are protected through consistent and proportionate regulation
- Remove the fees payable for social care providers to register with the Care Quality Commission (CQC), as the regulatory regime is primarily designed to provide public protection.
- Require CQC to assure the quality of all social care services, however they are delivered, including developing models which are currently outside the scope of existing regulation.
5. Digital transformation of homecare
- Government should provide significant investment to speed-up the implementation of digital technology to improve the efficiency and quality of homecare services, and to support people to live well and independently at home where technology could replace personal care.
6. Address long-term funding and publish a Social Care Green Paper
- The Social Care Green Paper was first announced in the Budget in March 2017. It is now well over two years since the announcement and, at the time of writing, there are no firm dates when it will be delivered. Work must be undertaken in this one-year spending round period to establish a longer-term solution to the funding of adult social care.
We accept that provision of additional funding to front-line homecare services will come at a cost.
However, there will be savings too as well as improvements in the delivery of homecare and efficiencies gained through health and social care systems working together.
We remain committed to working with Government to support a thriving social care system which supports those in receipt of state-funded care and those who fund their care from their private means.
Yours sincerely,
Colin Angel
Policy and Campaigns Director
Spending Review 2020-2021: Funding of homecare services
Invest in the social care workforce
1. Skills for Care estimate the number of homecare jobs in England in services regulated by the Care Quality Commission (CQC) to be 685,000 jobs (42% of the total), equivalent to the size of the residential care workforce.[1]
2. Government has no routine data collection of the relative proportions of homecare services purchased by the State and by private individuals, but our best estimate is that around 70% of homecare is purchased by the State; mostly by local government, and to a lesser extent by the NHS.
3. UKHCA therefore believes that the fees paid to homecare providers, by councils and the NHS, have the biggest impact on recruitment and retention of the workforce, and the overall financial viability of the homecare sector
4. The staff turnover rate was higher for domiciliary care providers in 2017-18 (the most recent year with published data) than other service types within social care. Over a third (36.8%) left their role within the previous 12 months. The turnover rate of front-line care workers was 42.3%, meaning around two in five left their role within the previous 12 months.[2]
5. The ability of social care employers to recruit and retain staff has been further exacerbated by the widening pay differentials between healthcare assistants employed in the NHS, and the pay of homecare workers in the independent and voluntary sector
6. In 2017-18, an NHS healthcare assistant could expect to receive £7.89 per hour; for careworkers, median pay in 2017-18 was £7.89 per hour, compared to the prevailing rate of the National Minimum Wage for workers aged 25 years and above which was £7.50 per hour.
7. Pay increases from 2018-19 in the NHS increased the rate a healthcare assistant could receive to £8.95 per hour. However, homecare providers, particularly those heavily dependent on local government funding, already struggle to compete with NHS colleagues based on the hourly rates paid by most local authorities and are at a further relative disadvantage in the labour market as a result.
8. In addition to the comparison of pay rates, above, NHS employees generally receive more advantageous pension and annual leave entitlements than are available in the independent and voluntary sector.
9. There is no doubt that homecare workers are undervalued by national and local government and society in general. Providing homecare to people who need support with personal care and other activities of daily living is repeatedly referred to as a ‘low skilled’ occupation, but this is far from the case.
10. Homecare workers also contribute to the economy as taxpayers; enable family carers to remain in employment and reduce stresses on the NHS by helping to avoid hospital admissions and facilitating safe hospital discharge.
11. With an increasingly older population experiencing multiple long-term health conditions, careworkers increasingly undertake roles previously delivered by community nurses, for example stoma-care; enteral feeding; and maintaining tissue viability.
12. While the Care Certificate, introduced in 2015, has standardised induction training for both homecare workers and healthcare assistants, the nature of social care services mean that employers often have much flatter career structures, with a far lower ratio of senior roles to those of front-line workers. We see very little evidence of councils purchasing services which enable a larger number of more senior roles to be available; in the majority of cases homecare services are purchased at a simple flat hourly rate, regardless of the skill or experience required to deliver the care required.
13. Homecare workers currently make up 42% of the adult social care workforce, the same proportion as residential care services. Skills for Care’s data modelling suggests that the number of social care jobs will need to increase by between 36% (580,000 jobs) and 50% (800,000 new jobs) by 2035. This is a total of between 2.2 and 2.42 million jobs.[3] Following a trend in government policy to support more people at home, increasingly higher proportions of this workforce will be in the homecare sector.
14. The need for homecare workers could be even greater than Skills for Care predict, if the Government’s own policies in the NHS Long-Term Plan to promote home-based care and prevent delays in hospital discharge is successfully implemented. Even if we assume our ageing population will, in the future, have fewer years of debilitating illness or disability, a quarter of the social care workforce is over 55 years old (320,000 jobs) and therefore, this group could retire within the next ten years.
Develop a workforce strategy and ensure future migration policy works for social care
15. The absence of a social care green paper means that a credible workforce strategy and plan is not in place. It needs to be developed – and arguably can be, even in the absence of a green paper.
16. A future workforce strategy should ensure there are sufficient properly-trained homecare workers, who can deliver the care people need to live independently in their own homes. This strategy and plan needs to explain how it matches and relates to the ambitions set out in the NHS Long Term Plan and the needs of people who are supported at home by local authority funded care and people who fund their own care.
17. The workforce strategy and the UK’s future migration policy after our exit from the European Union in October 2019 must also meet the combined impact of:
A) Fewer non-British EEA nationals coming to the UK since the EU Referendum;
B) Increasing numbers of non-British EEA nationals leaving the UK before Brexit;
C) The loss of Freedom of Movement immediately after the UK leaves the EU without a deal (or following a short transition period if leaving without a deal);
D) Increased labour market competition between social care, retail, hospitality and alternative employment sectors.
18. A widening polarisation within the homecare market will be an increasing trend if the workforce supply is not addressed. We detect a shift by care providers away from council contracts and towards the self-funded market (where more competitive fees can be charged).
19. UKHCA predict this situation will worsen as it becomes increasingly difficult to recruit staff. This will leave older and disabled people, particularly those whose care needs are supported by the State, in the position of having to wait even longer for the care they need, with the risk that rather than have care at home, admission to a care home becomes unavoidable.
Review the operation of apprenticeships for homecare workers
20. The apprenticeship levy is intended to increase the skills and training of the UK’s workforce by incentivising employers to use the levy they pay to offer apprenticeships. The requirement for workers to spend 20 percent of their working time in out-of-workplace training means that employers need to replace staff, for which they are not funded (wages being payable to two workers, only one of whom will generate revenue for the employer). Many homecare providers have reported that the out-of-workplace requirement is a considerable barrier to offering apprenticeships to front-line workers, and they are therefore unable to draw down monies from the levy.
21. Government should redesign the requirements for apprenticeships for mobile workers so that the apprenticeship levy is used to increase training, rather than effectively becoming a tax on social care employers.
A sustainable, vibrant and diverse homecare market
Invest in the social care market
22. Given that around 70% of homecare is state-funded, investment in a vibrant and diverse market must ensure local authorities have sufficient resources to pay the necessary fees so that providers can meet their legal and social responsibilities.
23. UKHCA’s report, “The Homecare Deficit 2018”,[4] showed that in 2018-19 the UK’s homecare sector needed £402 million to guarantee that homecare workers receive the Government’s statutory National Living Wage, whilst also enabling homecare providers to meet their statutory obligations. To ensure homecare services are financially stable, an additional £921 million was needed which would allow the entire workforce to be remunerated at the rate of the (voluntary) Living Wage, as independently calculated by the Living Wage Commission. Even this would do nothing to enable additional services to be delivered to the 1.4 million people currently believed to be living with unmet needs, many of whom would benefit from home-based care.
24. Since we published “The Homecare Deficit 2018”, we have re-calculated the size of the funding gap to reflect the increases in the NMW/NLW and employers’ contributions in workplace pensions in April 2018, as follows:
| Administration | Size of Deficit to meet UKHCA's Minimum Price of £18.93/hour | Size of Deficit to meet the (voluntary) UK and London Living Wage |
|---|---|---|
| England | £411,000,000 | £778,017,645 |
| Wales | £29,399,201 | £54,285,967 |
| Scotland | £86,811,287 | £152,918,627 |
| Northern Ireland | £71,354,369 | £96,185,144 |
| UK | £598,564,857 | £1,081,407,383 |
25. Without adequate funding the care market will remain economically unsustainable and more people will be affected by providers who are forced to hand-back contracts to councils or cease trading.
26. Under their duties of oversight of the social care market, CQC wrote to 84 local authorities warning them of the likely financial failure of Allied Healthcare, and estimated 9,300 older and disabled people were at risk of losing their homecare services after 30 November 2018.
27. Although the majority of Allied Healthcare’s services were subsequently transferred to CRG, and carried on trading, the fact that a major supplier of homecare came within days of ceasing business shows the fragility of the homecare market, and the risks to older and disabled people who rely on state funded care and support in order to live independently at home.
28. Allied Healthcare is the most recent (and extreme) example of potential market failures in the homecare sector, with a number of owners divesting themselves of their homecare services, often at a considerable loss.
29. Recent significant announcements from homecare providers have included:
- Care UK reported an operating loss on its homecare business and sold its services to Mears Group in June 2015.[5]
- Saga plc, which had previously owned Allied Healthcare, wrote down the value of the company to zero, in order to sell to the Aurelius Group in December 2015.[6]
- The Mitie Group plc wrote off the value of MiHomecare in March 2017 (prior to Apposite Capital’s acquisition of MiHomecare) and announced its withdrawal from the homecare sector.[7]
- Housing and Care 21 announced its intention to exit from the homecare market in September 2017, selling its homecare division to Core Capital (owners of Ark Healthcare).[8]
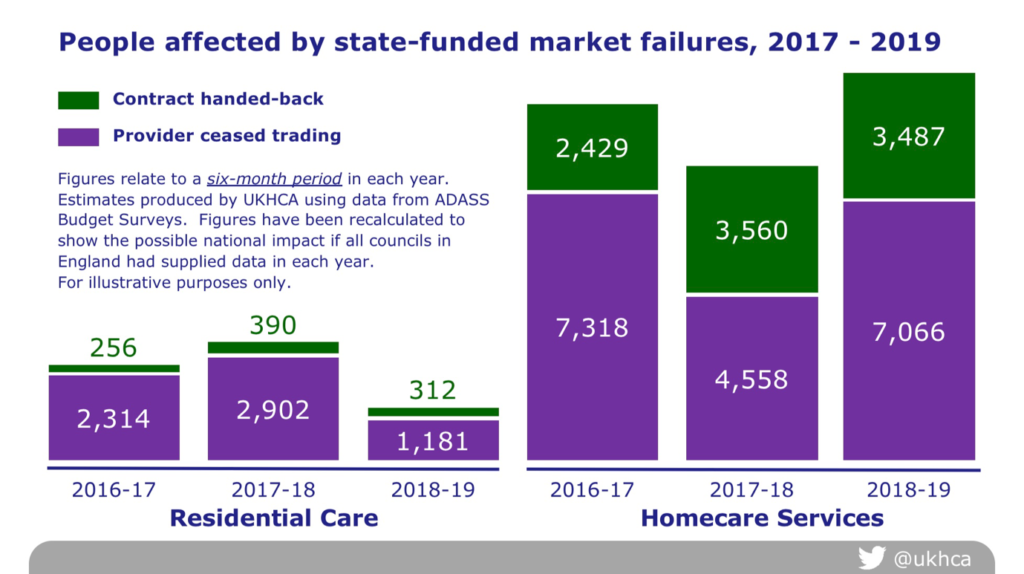
30. The Association of Directors of Adult Social Services Budget Survey 2019 reported that 72 (of 152) directors said they had seen homecare providers closing or ceasing to trade in the previous six months (impacting on 7,019 people) and 38 directors had seen contracts handed back by homecare providers (impacting on 3,464 people) in the same period.
31. We believe that the following graph shows that homecare providers are increasingly unwilling to accept the low fee rates offered by councils and the consequent risks of financial failure. As a result, increasing numbers of care packages are being handed back, and the numbers of people affected is increasing. This impact is significantly higher in the state-funded homecare sector than in residential care.
32. For homecare providers continuing to supply to councils, low prices paid for homecare services create unacceptable risks. These include:
- Poor terms and conditions for the workforce;
- Insufficient resources to organise the service; and
- Insufficient training for the complex work that supports the increasingly frail and disabled people who qualify for state-funded support.
33. There are a variety of reasons why the homecare sector is particularly vulnerable. UKHCA designed a research project to identify and prioritise the highest risks to the financial failure of provider organisations, or the risk to planned withdrawal from the provider market.[9] The views of homecare providers operating from 522 locations in the UK have been used to produce a ‘risk register’ for state-funded homecare services. These were supplemented by the views of providers from a further 282 locations who supply wholly or mainly to state-funded services. The following list summarises the risks to market stability in order of perceived risk by homecare providers:
- Inadequate fee levels
- Inadequate price increases
- Lack of engagement between authorities & providers
- Low, or inadequate, direct payments
- Ceiling prices in council contracts
- Spot purchase from non-framework providers
- Late payment of invoices
- Invoicing based on electronic call monitoring data
- Poor contract handover arrangements
- Risk-averse or disproportionate contract specifications
- Unrealistic expectations of TUPE transfers
- High use of short homecare visits
- Short contract lengths
- Restricted approved provider lists
- Use of unregulated care services
34. One provider responding to this survey said:
“The upward pressure of staff salaries and the downward pressure from council fees mean quality will suffer and recruitment, which is already difficult, will become an acute problem. We have already made significant cuts to our central and management costs; further savings will impact upon the quality of support and training we can offer our staff and the quality of the service we offer. Staff turnover will increase and the risk of not covering visits will increase dramatically.”[10]
Ensure funding is targeted at stabilising the provider market
35. Central government’s standard practice to fund social care is to increase funding to local government. Whilst in theory a proportion of this money can be used to promote the stability of social care markets, councils are also encouraged to use the available funds to cover their existing overspends or reduce delayed transfers of care.
36. Often this funding, such as the Better Care Fund, is made available for short periods of time, without a guarantee that they will be renewed. Authorities are generally reluctant to use the money in ways which might create a liability for them once the funding ceases.
37. Our member organisations report little evidence of councils using additional monies to stabilise the market by covering the additional financial burdens borne by providers, including increases to the National Living Wage and higher contributions to workplace pensions.
38. Government should ensure enough funding is available for adult social care overall. Where Government’s intention is that short-term funding should be used for stabilising the provider market, it should be ring-fenced and only approved where councils can demonstrate their plans to do so.
Require councils to establish the real cost of homecare with their providers
39. The prices which councils pay for homecare are frequently determined irrationally, and without an appreciation of the actual costs included. Generally, prices do not reflect the actual cost incurred, particularly in relation to local wage expectations, careworkers’ travel time and the costs of running the service.
40. Despite paragraphs 4.27 to 4.31 of the Care and Support Statutory Guidance, and guidance funded by Government for commissioners and published by CIPFA, the majority of councils are failing to recognise the actual costs of care and are increasing the instability of the sector. In a Freedom of Information Act enquiry in 2018, only one third (34%) of councils could demonstrate that they had examined the actual costs of care that year.[11]
41. Government should require councils to demonstrate that they have undertaken an open and transparent cost of care exercise with their local providers.
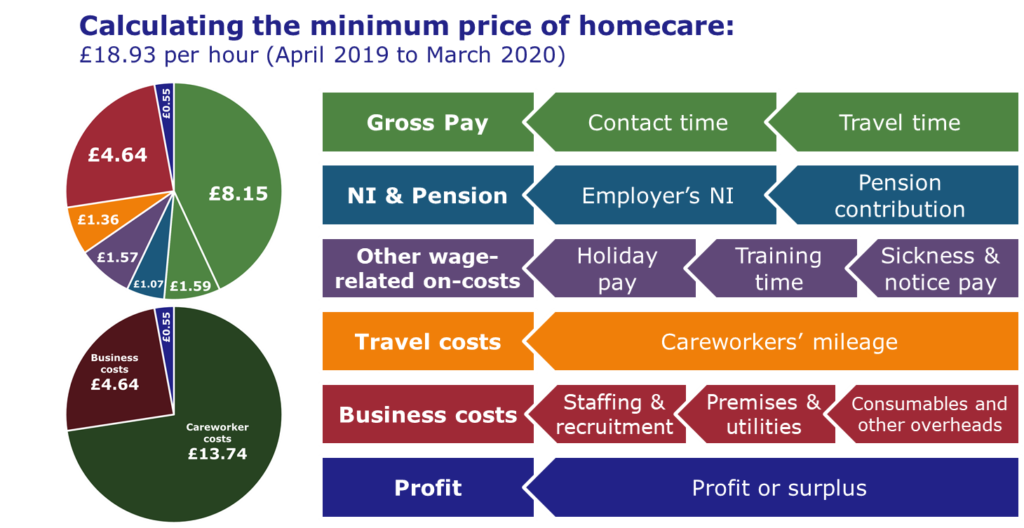
42. UKHCA have provided a number of tools to help authorities do so, including a detailed briefing on the calculation of the Minimum Price for Homecare, which from April 2019 is £18.93 per hour.[12] Government directs councils to UKHCA’s costing methodology in the Care and Support Statutory Guidance,[13] yet in recent months we have seen at least two councils tendering for homecare services in the region of below £15.00 per hour.
43. The minimum price for homecare is illustrated in the following simplified diagram:
Oversight of local authority commissioning practice
44. Although the Care Act 2014 places statutory duties on local councils in England, there is virtually no oversight of how authorities meet their market-shaping duties and no systematic review of this is in place. We believe that the Department of Health and Social Care is largely unaware of the reality of commissioning practices as most of the information the Department has comes from councils themselves.
45. As the statutory body with responsibility for regulating adult health and social care services in England, the Care Quality Commission (CQC) may be best placed to take on an oversight role, which was previously undertaken by CQC’s predecessor, the Commission for Social Care Inspection (CSCI). However, CQC is currently only able to report on the symptoms found in the current system; it is prevented by Government from examining the causes of market instability.
46. Although CQC would not necessarily need to be the body given such oversight responsibilities, it would be logical because CQC already holds a rich source of data about the quality of social care services delivered and operates at a distance from both local and central government and providers.
47. It is illogical, in our view, that Government should have established a regime of regulation of social care providers, but not have an oversight regime for the commissioning function of the majority purchaser of the sector’s services.
48. Oversight of local authority commissioning would be a way for Government to ensure that public money spent on social care is being well-used and reaching front-line services, where they are most needed.
Create a social care Market Oversight regime which covers local authorities
49. Government charged CQC with the operation of a market oversight regime. This assesses the financial viability of the largest social care providers and other providers whose services are categorised as “hard-to-replace”. However, this regime does not provide Government with a view on the potential for systemic failure in a local or regional market.
50. While we understand that the Department of Health and Social Care undertakes some monitoring of state-funded markets, there is no assurance for the public this activity is systematic, comprehensive or effective.
51. While we understand that the Department of Health and Social Care undertakes some monitoring of state-funded markets, there is no assurance for the public this activity is systematic, comprehensive or effective.
Funding homecare to reduce pressures on the NHS
52. We have seen over recent years increased pressures on the NHS over the winter period, and, during 2018, over the summer also. Homecare services should be particularly well placed to help deliver services which are designed to prevent illness or accidents amongst people with disabilities and frail older people.
53. People aged 80+ are most likely to attend A&E, and one in three emergency patients admitted for an overnight stay had five or more health conditions. As well as preventing avoidable hospital admissions, careworkers are also well placed to provide care for people being discharged home and providing or arranging help for people to regain independence. A person needing four hours of care at home would cost at a minimum rate £75.72 a day, whereas a stay in a hospital bed could cost in the region of £350 a day.
54. However, without sufficient investment in these areas, and unless there is a credible plan to deliver a health and social care workforce that has the right skills, pressures on the NHS are likely to continue to grow.
55. If such pressures are to reduce, we need a commissioning process that supports homecare provision together with independent oversight of commissioning practice of the public bodies purchasing care.
Take actions which reduce avoidable costs for social care providers
56. Several actions could be taken to ease the financial position of social care providers, if Government is willing to do so. These will enhance the effectiveness of additional funding from central government, including those outlined in this section. These items should be read in conjunction with our comments on CQC’s fee scheme for providers in England, which follows.
Change the VAT status of “welfare services”
57. At present, the VAT status of regulated homecare is “exempt” from VAT.[14] This means that the end-users of regulated care (councils, the NHS or private individuals) are not charged VAT, but regulated providers are unable to re-claim the VAT which they pay on the products and services they purchase in order to deliver that care.
58. Government should change the VAT status of “welfare services” from “exempt” to “zero-rated”, so that homecare providers can re-claim their input taxes.
59. Government has previously told us that membership of the European Union would prevent them from acting on VAT. The UK is now set to leave the European Union. This action could be a positive outcome resulting from the UK’s decision to leave the EU.
Resolve the risk of National Minimum Wage claims in relation to “sleep-in” duties
60. Social care providers using ‘sleep-in’ duties are currently back in a period of uncertainty while awaiting the outcome of a hearing in the Supreme Court on the interpretation of the National Minimum Wage Regulations.
61. We do not believe that it was ever Government’s intention that the National Minimum Wage would apply to workers while sleeping.
62. Government should confirm that it will underwrite the costs of any historic claims for sleep-in duties, to avoid extensive market failures during the next two to three years and to provide additional confidence to a fragile social care market, particularly for those which supply to people with a learning disability, where the use of ‘sleep-ins’ is particularly high.
63. Subject to the outcome of this hearing, Government should also undertake to clarify the legal position by making a clear amendment to the National Minimum Wage Regulations (rather than letting the matter rest on case-law).
Legislate to amend case-law on holiday pay
64. The decision of the Court of Appeal in The Harpur Trust v Brazel & Unison published on 6 August 2019 has made clear that employers can no longer legally calculate holiday based on 12.07% of hours worked over a year for those employed on permanent contracts of employment.
65. Judge Underhill concluded that employees who work for part of a year are entitled to receive a full 5.6 weeks paid annual leave at their average weekly remuneration in the 12 weeks preceding the holiday. This case is likely to have significant impact on the affordability of social care (and in other business sectors, such as education and retail), where zero hours contracts are used.
66. While Judge Underhill recognised the potential implications of his decision, he concluded that the Working Time Regulations did not provide for a pro-rating approach to holiday accrual for permanent staff.
67. We do not believe that the intention of the UK Parliament was for zero-hours employees to continue to accrue holiday when not working. We believe that Government should address the current legislation and provide a clear system for working out holiday pay for permanent zero-hours workers. In the meantime, Government should underwrite the costs of claims arising from members of the workforce for alleged underpayment of holiday pay in these situations.
Consistent and proportionate regulation
CQC registration fees
68. Homecare providers generally support registration and inspection and recognise that there is a cost to regulating adult social care. However, in April 2018, the Care Quality Commission (CQC) introduced a new method of calculating annual registration fees which had a far greater impact on homecare providers than other sectors.
69. The purpose of regulation is to protect and reassure the public. We therefore believe that Government should bear the costs of regulation directly, rather than pursue a scheme where financial burdens for providers are increased.
70. Whilst recognising Government’s policy requirement that the regulator must recover all its applicable costs from providers, the methodology employed by CQC to calculate fees for homecare providers is based on the number of service users supported and does not appear to equate the fee demanded with the actual costs of regulation.
71. If providers are to bear the costs of regulation then it is imperative that CQC demonstrate value for money in its regulatory activities and is confident that its fee regime does not exacerbate financial pressures within the sector.
72. The greatest impact of the fee changes has been on larger providers who have seen some fees increase by between 100% and 1,000% even though some very small providers, with 50 or fewer service users, will have seen more modest increases or, in some cases a reduction in fees over what was paid in 2017.
73. Although providers with 50 or fewer service users make up 65% of the market, the larger providers serve a greater number of service users and should a large provider fail the impact on the market will be far greater.
74. In our view, CQC’s imposition of the current fee structure has been rushed for two consecutive years and has left many service providers unable to budget effectively. This has increased the risk that those providing homecare may struggle, not just because their own costs have increased, but because of the massive fee increases demanded by CQC.
75. UKHCA now has examples where CQC’s fee scheme is already pushing stretched care providers to the brink and we have examples of providers being unwilling to deliver services to people with relatively small packages of care, as the per capita fee outweighs the revenue gained from delivering the service.
76. To illustrate this point, in 2017 CQC charged a flat rate registration fee of £2,192 per location. From April 2018 charges were based on the number of service users served by each location. Charges are based on the following formula £239 + (number of service users × 54.305) to a maximum fee of £92,558.
77. According to CQC’s data there are currently 5,703 registered homecare locations in England. CQC further groups those locations according to the number of service users served by each location. This means:
- Providers with 50 or fewer service users (3,769 providers) saw their fees rise to £2,528 – an increase of £336, or 15% above 2017/18 levels;
- Providers with between 50 and 100 service users (1,067 providers) saw their fees rise to £4,816, an increase of £2,624, or 120% above 2017/18 levels;
- Of the 657 providers with between 101 and 250 service users fees rose to £11,682 – an increase of £9,490 or 433% above 2017/18 levels;
- The 210 providers with more than 250 service users saw their fees rise to £21,000, or 1,000% over 2017/18 levels.
78. UKHCA has argued consistently that CQC should base its fees on a universal flat rate registration fee and with a proportionate charge for the actual costs of inspection and follow-up action.
79. No evidence has been provided that CQC has assessed the true impact of the fees’ structure on service provision nor provided evidence that the fees represent value for money. In our view, CQC has failed to provide convincing evidence that the fees’ structure currently in place meets CQC’s stated aim of aligning income to the actual costs of regulation (as opposed to CQC’s overall operating costs).
80. We urge Government to look again at the nature of the burdens placed on homecare providers by regulatory fees.
New and unregulated models of care
81. A change in the law to keep up with new models of care will be fairer to current providers and reassure the public that the care they receive has been inspected for quality and safety.
82. Currently the public has less protection if they employ or engage careworkers through private arrangements with individual care workers, or use organisations which solely introduce workers through the internet. Indeed, careworkers providing care to older and disabled people through a private arrangement are not required to submit any documentation to anyone. They are not ‘licensed’ nor required to register with a statutory body. This leaves an obvious gap in the protection of the public.
83. New, unregulated models of care include:
- Online employment agencies which claim to introduce self-employed careworkers to people paying for care from their own means, or with a direct payment. However, close examination of the workers’ job role mean that such claims of self-employment are likely to be spurious;
- Councils encouraging small numbers of personal assistants to join together to co-ordinate their services, crossing the threshold that should require registration with CQC, but without requiring the personal assistants’ arrangement to register;
- A scheme for people to offer their spare rooms as secure spaces for patients who are medically fit to be discharged from hospital, but are not ready to return to their own homes.
84. We are concerned about these new models of care because:
- there are no independent checks made on the quality of care or training received by the careworkers;
- there is no verification that criminal record checks are being carried out;
- nor are there checks on whether the careworker has been legally barred from working with vulnerable people.
Digital transformation of homecare
85. Government should provide significant investment to speed-up the implementation of digital technology to improve the efficiency and quality of homecare services.
86. Technology can also be used to support people to live well and independently at home, where support can be managed without the need for personal care provided by individual workers.
Long-term funding of care and the Social Care Green Paper
87. Government has been committed to the publication of a social care green paper and the Prime Minister, on his first day in office, announced that:
"My job is to protect you or your parents or grandparents from the fear of having to sell your home to pay for the costs of care.
“And so I am announcing now – on the steps of Downing Street – that we will fix the crisis in social care once and for all, and with a clear plan we have prepared to give every older person the dignity and security they deserve.”
88. Finding a solution for the funding of social care has proved intractable and politically perilous for both Labour and Conservative governments in recent years.
89. The ambition should not be solely one of protecting the housing assets of those who have them, but of developing a system which is fair and equitable.
90. In addition, many disabled adults of working age do not own their own homes, or if they do, it would be inappropriate for them to move into a residential care facility. Services for working age adults account for approximately half of councils’ spending on social care, and is set to double by 2040.
91. Longer-term plans, beyond a spending round covering the next 12 months, must consider not only the support delivered to people supported by the state, but also those who fund their own care. These are matters which we have previously discussed with the Department’s Green Paper team, and will not rehearse them here.
92. Government must therefore continue to develop cross-party agreement on the content of such proposals which will gather enough support from across the political spectrum to be passed into law.
93. UKHCA wishes to confirm our long-standing support to any government willing to tackle this objective. Until such proposals are published, however, the current spending-round must support the social care sector to meet the needs of older and disabled people.
____________________________________________________________________________________
Footnotes
[1] Skills for Care (2019) The Size and Structure of the Adult Social Care Sector and Workforce in England, 2019, page 26.
[2] Skills for Care (2018) The State of the Adult Social Care Sector and Workforce in England, September 2018, page 35.
[3] Skills for Care (2019) The size and structure of the adult social care sector and workforce in England, 2019, section 7.
[4] https://ukhca.pixl8-uat.cloud/resource/the-homecare-deficit-2018.html
[5] www.healthinvestor.co.uk/ShowArticle.aspx?ID=4123.
[6] www.healthinvestor.co.uk/ShowArticle.aspx?ID=4505.
[7] www.telegraph.co.uk/business/2017/03/01/mitie-sells-healthcare-business-just-2/ and www.appositecapital.com/case-studies/mc-care-holdings/.
[8] www.communitycare.co.uk/2016/09/15/biggest-profit-provider-pulls-home-care-market/.
[9] Angel, C (2018) A Risk Register for State-Funded Homecare. URL: https://ukhca.pixl8-uat.cloud/resource/a-risk-register-for-state-funded-homecare.html.
[10] Comment from the owner of a single-site homecare provider in the West Midlands.
[11] Angel, C (2018) The Homecare Deficit 2018. A Report on the Funding of Older People’s Homecare Across the United Kingdom, page 92. URL: https://ukhca.pixl8-uat.cloud/resource/the-homecare-deficit-2018.html.
[12] Angel, C (2019) A Minimum Price for Homecare, version 6.0. URL: https://ukhca.pixl8-uat.cloud/resource/a-minimum-price-for-homecare-2021-2022.html. (Note: The Minimum Price for Homecare is a figure produced annually. At the time of writing this Blog, the Minimum Price for Homecare for April 2019 to March 2020 was £18.93. Version 6 has been superseded.)
[13] HM Government (2018) Care and Support Statutory Guidance, updated 26 October 2018, paragraph 4.31. URL: https://www.gov.uk/government/publications/care-act-statutory-guidance/care-and-support-statutory-guidance#chapter-4.
[14] HM Government (2011) Welfare services and goods (Notice 701/2). See: www.gov.uk/guidance/welfare-services-and-goods-notice-7012.
This blog was produced when the Homecare Association was known as UKHCA.





