Jane Townson, Chief Executive
Summary
Over the last two months, members of United Kingdom Homecare Association (UKHCA) have expressed growing alarm and concern about inadequate workforce capacity to meet demand for home-based support and care.
Many employers say they have never experienced such difficulty in retention and recruitment and fear for the well-being and safety of older and disabled people.
Providers’ concerns have been echoed by the Association of Directors of Adult Social Services in their Spring Survey 2021.

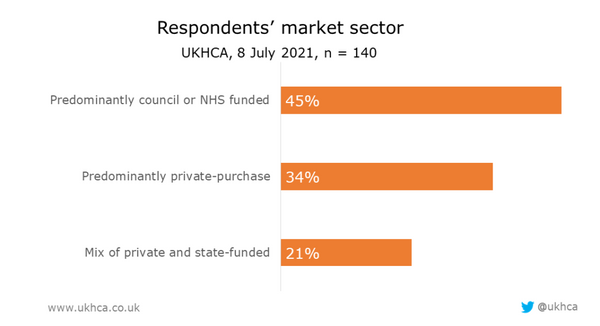
To obtain feedback from a wide range of homecare providers on current workforce pressures, we conducted a survey of UKHCA members on 8 July 2021.
Responses were received from 140 homecare providers, from small and medium enterprises to the largest organisations. Respondents represented a mix of state-funded and private-pay providers.
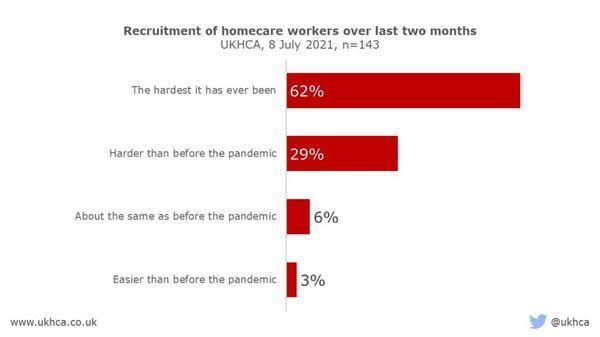
Of those who took part, 91 per cent said that recruitment is harder now than before COVID-19, or the hardest it has ever been.
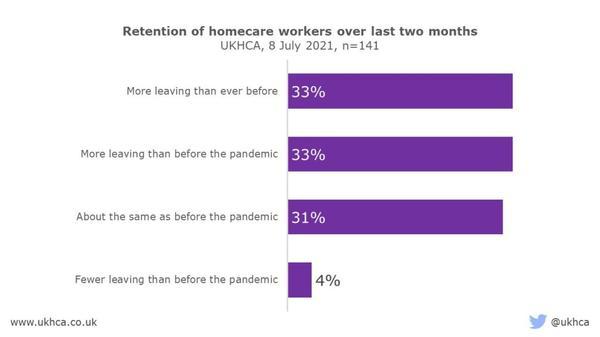
Difficulty recruiting homecare workers is particularly worrying, as two-thirds of providers reported that more careworkers are leaving their roles than before the pandemic, or more often than the employers could ever remember. Hardly anybody thought retention rates had improved.
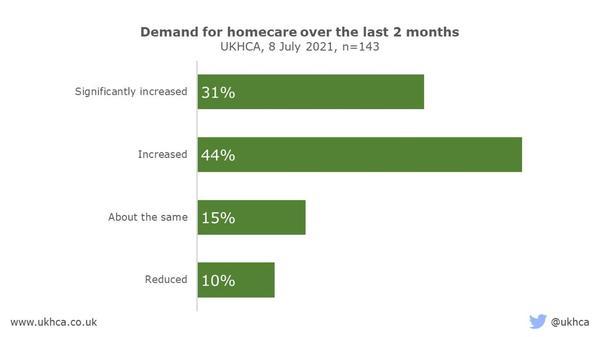
Three quarters of homecare providers surveyed said demand for their services had increased, or significantly increased, in the last two months.
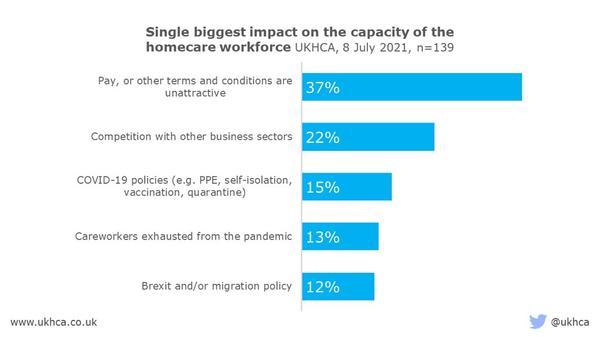
Many factors affect capacity of the homecare workforce. Our survey highlights that inadequate funding, which affects careworkers’ pay, terms and conditions of employment, and the way that homecare is commissioned and purchased, has a significant negative impact.
Competition with other business sectors, such as hospitality and retail; COVID-19 and associated policies; and migration policy are also having a detrimental effect on number of homecare workers available.
These influences on workforce capacity are discussed, as well as potential solutions.
To avoid harm to older and disabled people through inability to provide care and support services, we call on the government to take urgent action to address these issues as follows:
Immediate policy changes needed
- Revise migration policy with urgency by:
- Adding all careworkers to the Shortage Occupation List and reducing the salary threshold for immigration;
- Waiving the Immigration Skills Charge for careworkers, reducing the cost of obtaining the legal Right to Work for careworkers.
- Clarify and update the official guidance on “Management of staff and exposed patients or residents in health and social care settings” to reflect the new self-isolation guidance for health and careworkers, to avoid confusion. Self-isolation requirements are having a major adverse impact on workforce capacity at present, so the change is welcome. It is, however, unclear how workable it will be in the short-term for local public health teams to authorise all risk assessments.
- Review restrictions on movement between care settings of double-vaccinated and tested careworkers, assessing relative risks, to limit careworkers leaving jobs in social care for employment in the NHS, as is happening at present.
- Consider exemption from quarantine for live-in careworkers arriving in the UK from outside the Common Travel Area, provided they are double-vaccinated, PCR-tested, and without symptoms of COVID-19. It is important to balance the mitigated risk of infection with that to the safety and well-being of highly dependent older or disabled people being left without care. Current quarantine arrangements are significantly reducing the willingness of careworkers to travel to the UK, particularly from EEA and EU countries.
- Recognise legitimate vaccination certificates of careworkers from outside the UK, in addition to those supplied by the NHS. Current rules are unnecessarily impeding recruitment of fully vaccinated careworkers from overseas.
- Drop proposals for a requirement on social care providers only to deploy staff who are fully vaccinated, in favour of a voluntary approach to vaccination of homecare workers. Combine this with support for services with a higher proportion of vaccine hesitant staff; for example, funding health professionals and community leaders to support employers with careworkers who are vaccine-hesitant.
- Release targeted Workforce Capacity funding, paid directly to employers, which enables care providers to pay enhancements to staff to encourage them to remain in the care sector, rather than move to hospitality or retail.
- Re-invigorate the national recruitment campaign for careworkers.
- Provide bonuses of £500 per careworker to thank them for their extreme dedication and service at a time of national emergency, as has already happened in Scotland, Wales and Northern Ireland.
- Recognise homecare in internal and public communications. Doing so costs nothing and makes a huge positive difference.
- Fund occupational health support for careworkers, as is available for NHS staff.
Long-term policy reform required
- Fund social care adequately so that homecare workers are paid fairly for the skilled roles they perform, and at least on a par with equivalent public sector roles.
- End the practice of councils and the NHS of purchasing homecare “by-the-minute”, alternatively focusing on achieving the outcomes people want.
- Support development of an expert-led workforce strategy for social care and a 10-year workforce plan, aligned with the NHS People Plan.
- Create a professional register for careworkers in England, covering all paid social care workers in both regulated and unregulated care services. Registration of careworkers needs to be adequately funded and carefully implemented.
Survey of homecare providers
To obtain feedback from a wide range of homecare providers on current workforce pressures, we conducted a survey of UKHCA members on 8 July 2021.
Responses were received from 140 homecare providers, from small and medium enterprises to the largest organisations. Respondents represented a mix of state-funded and private-pay providers.
Results of survey
Recruitment and retention
Homecare providers surveyed told UKHCA just how difficult recruitment and retention of homecare workers has become in recent months. 91 per cent said that recruitment is harder now than before COVID-19, or the hardest it has ever been.
Difficulty recruiting homecare workers is particularly worrying, as two-thirds of providers reported that more careworkers are leaving their roles than before the pandemic, or more often than the employers could ever remember. Hardly anybody thought retention rates had improved.
Demand for homecare services
It is essential that older and disabled people who choose to live independently at home have careworkers who can support them.
Three quarters of homecare providers surveyed said demand for their services had increased, or significantly increased, in the last two months.
Factors influencing workforce capacity
Many factors affect capacity of the homecare workforce. Our survey highlights that inadequate funding, which affects careworkers’ pay, terms and conditions of employment and the way that homecare is commissioned and purchased, has a significant negative impact.
Competition with other business sectors, such as hospitality and retail; COVID-19 and associated policies; and migration policy are also having a detrimental effect on number of homecare workers available.
These influences on workforce capacity are discussed in more detail below.
Discussion
Most of us want to live well at home and thrive in our communities, regardless of age or disability. Many older and disabled people can live at home independently, with the support of family, friends and professional careworkers.

Failure to support older and disabled people with needs in their own homes risks avoidable deterioration in their health and well-being. This can result in crisis admissions to hospital or care homes, which are distressing for the individual concerned, costly for the state and may lead to further decline in function.
Analysis by Age UK found that, in the 12 months to February 2020, about 700,000 requests for formal care and support, equivalent to 51 per cent of all requests, were made by older people and yet resulted in them not receiving formal care services. This is equivalent to 2,000 claims from older people being unsuccessful each day, or 80 every hour.
We need a well-supported homecare sector, which has sufficient capacity to provide the services we expect to be available when we need them. This has benefits for individuals and their families as well as the wider health and care system.
Jobs in domiciliary care are increasing
Skills for Care data (2021) show that jobs in domiciliary care have continued to increase over the last decade, whilst jobs in residential care appear to have reached a plateau.
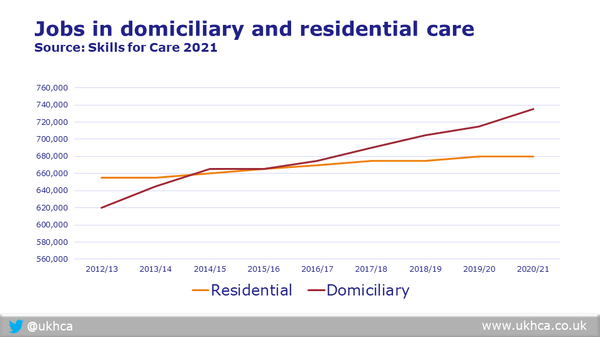
Despite the increase in jobs, demand for homecare is far out-stripping supply.
Demand for homecare is rising
Homecare providers are reporting that demand for homecare is rising in both the publicly and privately funded parts of the market.
In addition to normal demographic pressures, this appears to be due to a combination of pent-up demand in the community following the pandemic; informal carers being unable to cope; hospitals seeking to deal with backlogs of elective cases; and public concerns about safety and accessibility of loved ones in care homes.
A recent report by the Association of Directors of Adult Social Services (ADASS) warned that almost 75,000 disabled and older people, and carers, are waiting for help with their care and support. Adult social services are facing a deluge of requests for help as restrictions lift after COVID-19.
Councils say that informal care arrangements are breaking down; more people are seeking help with mental health issues or escaping from domestic violence; more people need support while waiting for hospital admission and more people need support after hospital discharge.
Unfortunately, all the signs are that the mismatch between demand and supply of homecare is worsening.
This is resulting in an increase in unmet need, people being placed in care homes when they could have gone straight home with support, and delayed discharges from hospital. Almost inevitably, this will create additional pressures in the NHS, at a time when COVID-19 cases and associated admissions are multiplying, and there is an estimated hospital waiting list of 13 million.
Providers are reporting that their difficulties in retaining and recruiting careworkers, even to maintain existing volumes, never mind to expand services, are currently more severe than they can remember.
Why are we in this position and what could be done to address the issues?
Long-term and short-term issues affecting workforce capacity are discussed below and solutions suggested.
Systemic issues affecting social care workforce
The systemic issues faced by our homecare workforce are well documented, and include:
- Poor pay, terms and conditions of employment, which do not adequately reflect the skills and experience required to support people with high dependency and complexity of need in the community;
- Inadequate investment in training, supervision and employee experience; and
- A lack of professional respect and agency.
All of these have dogged the sector for years, resulting in high vacancy rates and staff turnover.
A recent research report from Community Integrated Care, entitled Unfair to Care, suggests that many social care workers would be paid up to 39 per cent more – an additional £7,000 p.a. – if they worked in roles of equivalent skills and size in other public funded sectors.
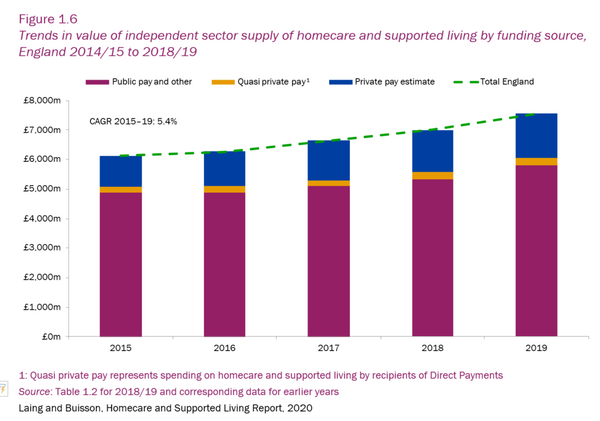
Laing and Buisson estimate that most hours of homecare delivered are purchased by public sector commissioners in councils, and to a lesser extent the NHS, who rely on central government funding for services. Private purchase of homecare is, however, steadily increasing. No reliable data are available on the latter and the total could be higher.
The employment conditions of a majority of careworkers in the state-funded part of the market result directly from inadequate central government funding for councils. This leads to poor commissioning and procurement practices, such as buying homecare by the minute, for contact time only. To make matters worse, many councils fail to acknowledge additional time spent by careworkers with care recipients, over and above what was commissioned. Per minute billing is thus often a one-sided arrangement in favour of councils, at the expense of careworkers.
Under-funding also risks inadequate investment in training, supervision and support of careworkers. This adds to their sense of professional insecurity and personal risk, which is already heightened due to lone-working in a heavily regulated sector.
These issues collectively create risks to the quality of care, as well as to the experience of both recipients of care and careworkers.
Valuing and investing in homecare and our workforce
We call on the government to value and invest adequately in homecare, viewing it as key to their ambition for the nation’s health:
“for everyone to have five extra years of healthy, independent life by 2035 and to narrow the gap between the richest and the poorest”.
Supporting people at home helps to shift the demand curve and reduces utilisation of more expensive health or residential care services.
Research conducted by Newcastle University and partners demonstrates that early intervention to maintain function of older people delays and compresses the time that care is required, improving quality of life and reducing costs.
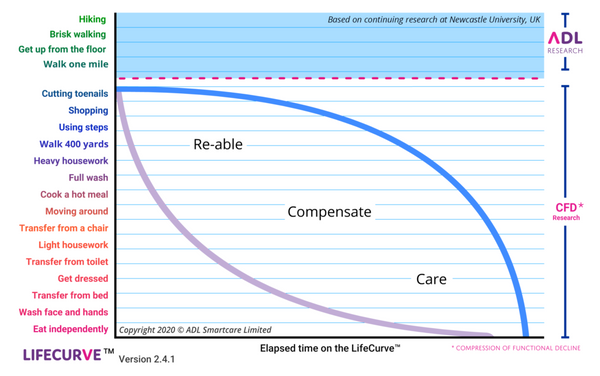
Shifting the demand curve has been demonstrated in practice by Eclipse Homecare, a UKHCA member in Worcestershire, where the council is now seeking to roll this approach out more widely.
Funding, commissioning and provision of homecare services are inextricably linked. In turn, they affect the capacity and stability of the workforce, as well as the quality of care.
We call on the government to:
- Fund social care adequately so that homecare workers are paid fairly for the skilled roles they perform, and at least on a par with equivalent public sector roles.
- End the practice of councils and the NHS purchasing homecare “by-the-minute”, alternatively focusing on achieving the outcomes people want.
A workforce strategy for social care
We call on the government to support development of an expert-led workforce strategy for social care and a 10-year workforce plan, aligned with the NHS People Plan. This requires a number of steps:
- Analysis of current and projected needs of older and disabled people, recognising that many are ageing with multiple, complex, long-term conditions.
- Definition of the skills, competencies and experience required of careworkers to meet these needs.
- Provision of funded and nationally recognised training, and qualifications (where necessary), to ensure careworkers develop the skills and competencies required to perform their roles.
- Fair recognition and reward for the varied levels of skill, competency and experience required for careworkers to perform different roles.
- Creation of a professional register for careworkers, covering all paid social care workers in both regulated and unregulated care services. A registering body would issue a Licence to Practice, which:
- Gives credibility to the profession;
- Promotes the status of care workers;
- Improves quality of care;
- Sets standards of ethics, conduct, and competence;
- Sets standards of training and development;
- Provides commitment to continuous professional development;
- Increase the skills and qualification levels across the workforce;
- Increases confidence of care workers;
- Ensures employers are accountable for effective training and developing staff;
- Provides important benefits to the members, such as advice and support, ability to share best practice, opportunities to network;
- Protects the rights of members; and importantly
- Protects the public from unqualified, incompetent or unfit practitioners, for example, by handling complaints and investigating and deciding on fitness to practise issues.
Crucially, though, a workforce strategy and plan of this nature, leading to professionalisation of care, needs adequate funding, and careful implementation to avoid unintended consequences. For example, careworker registration could create a risk of reducing the number of people applying for roles in care or delaying recruitment processes.
Negative impact on workforce capacity of more recent changes in government policies
Against this backdrop of long-term systemic issues, we have more recent changes in government policy and the operating environment, which are exacerbating problems with homecare workforce capacity, including:
- A reduction in workers from the European Economic Area (EEA) and European Union (EU) joining or continuing in the sector, as a result of change in migration policy following the UK’s exit from the EU;
- COVID-19 related policies and guidance, particularly:
- Self-isolation;
- Restrictions on staff movement between care settings;
- Travel restrictions and quarantine arrangements;
- Prospect of compulsory vaccination.
- Competition from wider labour markets, particularly hospitality and retail.
- Workforce exhaustion and disillusionment with the care sector.
EU exit and migration
Whilst the sector welcomed the addition of senior careworkers to the Shortage Occupation List, many providers do not receive sufficient fee rates from public sector commissioners to pay for the higher wages and immigration skills charge required, though the visa fee is reduced for health and care workers.
After paying for the certificate of sponsorship for a specific number of vacancies, the cost to obtain the legal Right to Work in the UK amounts to over £1000 per careworker.
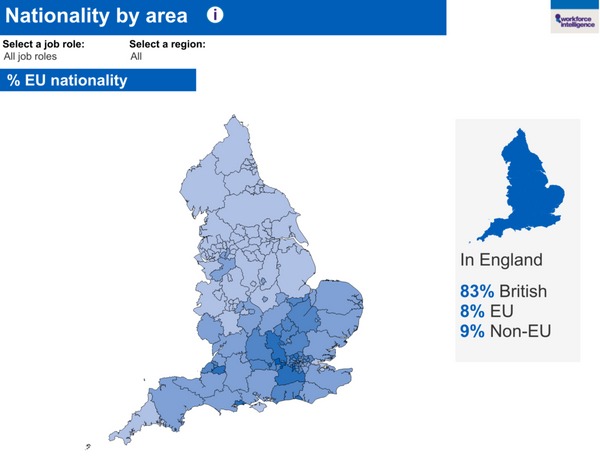
Regional differences in the proportion of EU nationals in the social care workforce, as described by Skills for Care, mean that the impact of reduced EU migration is felt particularly severely in London and the south east, as well as in urban centres elsewhere in the country.
The UK government talks about a home-grown care workforce. The reality is that, in some areas, no British nationals have come forward to apply for advertised jobs and staffing key services is almost wholly reliant on careworkers from abroad. Cutting off this supply is having a serious impact on services, particularly in some parts of the country.
The Migration Advisory Committee has been commissioned to undertake an independent review of adult social care, and the impact that ending freedom of movement has had on the sector.
This review follows a Government commitment given in the House of Lords during consideration of the Immigration and Social Security Co-ordination (EU Withdrawal) Act 2020 to look at the impact on:
- the adult social care workforce (such as skills shortages) covering the range of caring roles in adult social care including care workers, registered nurses and managerial roles;
- visa options for social care workers;
- long term consequences for workforce recruitment, training and employee terms and conditions; and
- any other relevant matters the independent chair deems appropriate which are relevant to the above three objectives.
This review, whilst welcome, will not report until April 2022, which will be too late to address immediate issues.
We call on the government to:
- Add all careworkers to the Shortage Occupation List and reduce the salary threshold; and
- Waive the Immigration Skills Charge for careworkers, reducing the cost of obtaining the legal Right to Work for careworkers.
COVID-19 related policies and guidance
Whilst everyone in the health and care sectors appreciates the vital importance of infection prevention and control, we need to balance risks.
Right now, the risks of being unable to support highly dependent older and disabled people due to workforce shortages have substantially increased. Key reasons for this are discussed below.
Self-isolation
Transmission rates of COVID-19 are continuing to rise, exacerbated by new highly transmissible variants and greater social contact, for example the return of children to school.
Government plans to implement stage 4 of the COVID-19 roadmap on 19 July 2021, lifting many restrictions originally designed to reduce transmission. For example, people will be left to make their own decisions about social distancing and use of face coverings. This is likely to lead to further increase in COVID-19 in communities, despite the successful roll-out of the vaccination programme.
Current government guidance requires immediate self-isolation for up to 10 days if:
- you have any symptoms of COVID-19 (a high temperature, a new, continuous cough or a loss or change to your sense of smell or taste);
- you have tested positive for COVID-19;
- someone you live with has symptoms or tested positive;
- someone in your childcare or support bubble has symptoms and you have been in close contact with them since their symptoms started or during the 48 hours before they started;
- someone in your childcare or support bubble tested positive and you have been in close contact with them since they had the test or in the 48 hours before their test;
- you have been told by NHS Test and Trace or the NHS COVID-19 app that you have been in contact with someone who tested positive;
- you have arrived in England from abroad (not including Ireland, the Channel Islands, the Isle of Man or other parts of the UK) and are not exempt from quarantine.
Due to rising community transmission rates, numerous careworkers are receiving notifications from the NHS COVID-19 app and NHS Test and Trace to self-isolate for 10 days.
In reports we have received from some services in recent weeks, over half of careworkers are currently unable to work due to self-isolation rules, which is severely limiting care and support available for older and disabled people.
The government announced on 19 July 2021 that, with immediate effect, double vaccinated front-line NHS and social care staff in England who have been told to self-isolate may be permitted to attend work, in exceptional circumstances, provided that daily testing is undertaken. Risk assessments must be conducted and authorised by the organisation’s local Director of Infection Prevention and Control, the lead professional for health protection, or the Director of Public Health relevant to the organisation.
Whilst welcome, the official guidance on management of staff or exposed patients or residents in health and social care settings has not yet been updated, creating confusion. It is unclear how workable it will be in practice for local health protection teams to manage all requests for authorisation in the short-term, given that many services are severely affected by staff shortages at present.
We call on the government to:
- Clarify and update the official guidance on “Management of staff and exposed patients or residents in health and social care settings” to reflect the new self-isolation guidance for health and careworkers, to avoid confusion. Self-isolation requirements are having a major adverse impact on workforce capacity at present, so the change is welcome. It is, however, unclear how workable it will be in the short-term for local public health teams to authorise all risk assessments.
Restrictions on staff movement between care settings
With a view to limiting spread of COVID-19, the government has introduced restrictions on movement of staff between care settings. This is understandable from the perspective of infection prevention and control but, again, we need to balance risks.
Nurses who previously did shifts in both the NHS and care services have chosen to work in the NHS.
There is also evidence of staff leaving the care sector for jobs in the NHS, where they are also experiencing staff shortages and can offer better pay, terms and conditions of employment.
We call on the government to:
- Release targeted Workforce Capacity funding, paid directly to employers, which enables care providers to pay enhancements to staff to encourage them to remain in the care sector.
- Review restrictions on movement between care settings of double-vaccinated and tested careworkers, assessing relative risks, to limit careworkers leaving jobs in social care for employment in the NHS, as is happening at present.
Travel restrictions and quarantine arrangements
International travel has been disrupted, which has affected everyone, including careworkers seeking to travel to the UK for work.
Quarantine rules have caused particular problems for the live-in care sector, which supports over 10,000 highly dependent people 24/7 in their own homes, and relies heavily on workers from Europe and beyond.
Some UKHCA members are paying the £1750 fee for the quarantine hotel, as well as £210 per person for border control tests, but careworkers are still declining to come, as they do not want to be confined for 10 days.
The most recent change to the UK government’s quarantine rules allows people who have been fully vaccinated with an NHS administered vaccine, plus 14 days, to travel to amber list countries without having to quarantine on their return to England, from Monday 19 July 2021.
From an infection control perspective, the logic of allowing some people to travel abroad and return without quarantine, and not others, is unclear.
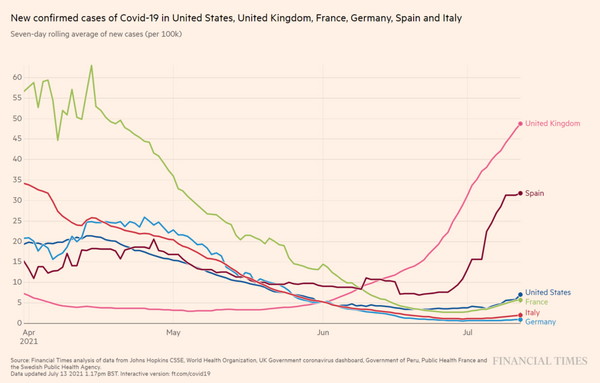
Given that the UK now has a higher COVID-19 transmission rate than any of our European neighbours, arguably there is a greater risk from domestic than from overseas travel.
Furthermore, it is unclear why those who have legitimate vaccination certificates from other countries, are excluded. Current rules are unnecessarily impeding recruitment of fully vaccinated careworkers from overseas.
Infection levels in registered live-in care services remain low and the live-in care hub also reports low death rates from COVID-19.
Providers consider the risks of being unable to supply care to those who need 24/7 support to be higher than the risk of infection from double-vaccinated and tested careworkers. Most work regularly with the same clients, enabling continuity of care, which is valued by recipients of services.
We call on the government to:
- Consider exemption from quarantine for live-in careworkers arriving in the UK from outside the Common Travel Area, provided they are double-vaccinated, PCR-tested, and without symptoms of COVID-19. It is important to balance the mitigated risk of infection with that to the safety and well-being of highly dependent older or disabled people being left without care. Current quarantine arrangements are significantly reducing the willingness of careworkers to travel to the UK, particularly from EEA and EU countries..
- Recognise legitimate vaccination certificates of careworkers from other countries, in addition to those supplied by the NHS. Current rules are unnecessarily impeding recruitment of fully vaccinated careworkers from overseas.
Prospect of compulsory vaccination
UKHCA strongly supports the vaccination of homecare workers against COVID-19. We have, however, clearly stated that our preference for now is to continue to encourage voluntary uptake of vaccination.
We fear that compulsory vaccination will exacerbate workforce shortages, particularly in London and the southeast, where vaccine hesitancy is highest.
In many cases, the kind and patient approach adopted by employers, GPs, nurses and pharmacists when talking directly to those who have concerns, has been instrumental in influencing individuals to accept vaccination.
We call on the government to:
- Drop proposals for a requirement on social care providers only to deploy staff who are fully vaccinated, in favour of a voluntary approach to vaccination of homecare workers. Combine this with support for services with a higher proportion of vaccine hesitant staff; for example, funding health professionals and community leaders to support employers with careworkers who are vaccine-hesitant.
Competition from the wider labour market
Due to travel restrictions, more people are booking holidays in the UK. Prices of accommodation are escalating in some places, allowing employers in the hospitality sector to pay bonuses and much higher wages than the care sector. This is having an adverse effect on recruitment and retention of careworkers in some areas.
Despite this, employers in the retail and hospitality sectors are also reporting labour shortages. They, too, are likely experiencing an impact of lower inward migration since the UK’s exit from the EU.
We call on the government to:
- Deliver on their promise to reform social care and fund it adequately, so that careworkers are paid fairly compared with other public sector jobs;
- Release targeted Workforce Capacity funding, paid directly to employers, which enables care providers to pay enhancements to staff to encourage them to remain in the care sector, rather than move to hospitality or retail.
- Re-invigorate the national recruitment campaign for careworkers.
Workforce exhaustion and disillusionment with the care sector
Careworkers and care leaders have worked tirelessly throughout the pandemic, many without adequate rest. Unlike their counterparts in the NHS, there is little meaningful recognition from government or the public.
Careworkers in Scotland, Wales and Northern Ireland have all been given bonuses of £500. In Scotland this has been done twice. In England there has been nothing.
Whilst the public lauds the NHS, which received the George Cross, social care, particularly homecare, tends to be ignored.
Worse still, the care workforce in England is experiencing central government’s approach towards them as negative and punitive. For example, rather than choosing to work with the sector to encourage those who are vaccine hesitant to obtain their jabs voluntarily, as advised, the government is rushing through ill-considered secondary legislation to enable compulsion (initially in care homes), without an Impact Assessment or analysis of the practicalities of implementation.
Meanwhile, some local authorities have reportedly threatened homecare providers with breach of contract for being short of staff, though the causes of this are largely out of their control, as outlined in previous sections.
Solicitors say they are seeing increasing numbers of prosecutions of providers by the Care Quality Commission and a more negative style of inspection, where the goal appears to be to find fault rather than to support improvement.
At CEO and director level, there seems to be a growing number of resignations, as well as business sales. Leading in this environment is perceived to be a thankless and almost impossible task.
We call on the government to:
- Provide bonuses of £500 per careworker to thank them for their extreme dedication and service at a time of national emergency, in line with the devolved administrations;
- Recognise homecare in internal and public communications. Doing so costs nothing and makes a huge positive difference;
- Fund occupational health support for careworkers, as is available for NHS staff.
Summary of urgent actions required
Homecare providers all over the country, regardless of size, type or location, are reporting more severe difficulties with recruitment and retention of careworkers than ever before.
It is hard to maintain existing workforce capacity, never mind grow to meet rising demand for homecare.
Numerous short- and long-term issues affecting the care workforce have combined to create a situation of high risk for older and disabled people.
Urgent action is required by the government to address these issues as follows:
Short-term policy changes
- Revise migration policy with urgency by:
- Adding all careworkers to the Shortage Occupation List and reducing the salary threshold for immigration;
- Waiving the Immigration Skills Charge for careworkers, reducing the cost of obtaining the legal Right to Work for careworkers.
- Clarify and update the official guidance on “Management of staff and exposed patients or residents in health and social care settings” to reflect the new self-isolation guidance for health and careworkers, to avoid confusion. Self-isolation requirements are having a major adverse impact on workforce capacity at present, so the change is welcome. It is, however, unclear how workable it will be in the short-term for local public health teams to authorise all risk assessments.
- Review restrictions on movement between care settings of double-vaccinated and tested careworkers, assessing relative risks, to limit careworkers leaving jobs in social care for employment in the NHS, as is happening at present.
- Consider exemption from quarantine for live-in careworkers arriving in the UK from outside the Common Travel Area, provided they are double-vaccinated, PCR-tested, and without symptoms of COVID-19. It is important to balance the mitigated risk of infection with that to the safety and well-being of highly dependent older or disabled people being left without care. Current quarantine arrangements are significantly reducing the willingness of careworkers to travel to the UK, particularly from EEA and EU countries.
- Recognise legitimate vaccination certificates of careworkers from outside the UK, in addition to those supplied by the NHS. Current rules are unnecessarily impeding recruitment of fully vaccinated careworkers from overseas.
- Drop proposals for a requirement on social care providers only to deploy staff who are fully vaccinated, in favour of a voluntary approach to vaccination of homecare workers. Combine this with support for services with a higher proportion of vaccine hesitant staff; for example, funding health professionals and community leaders to support employers with careworkers who are vaccine-hesitant.
- Release targeted Workforce Capacity funding, paid directly to employers, which enables care providers to pay enhancements to staff to encourage them to remain in the care sector, rather than move to hospitality or retail.
- Re-invigorate the national recruitment campaign for careworkers.
- Provide bonuses of £500 per careworker to thank them for their extreme dedication and service at a time of national emergency, as has already happened in Scotland, Wales and Northern Ireland.
- Recognise homecare in internal and public communications. Doing so costs nothing and makes a huge positive difference.
- Fund occupational health support for careworkers, as is available for NHS staff.
Long-term policy reform required
- Fund social care adequately so that homecare workers are paid fairly for the skilled roles they perform, and at least on a par with equivalent public sector roles.
- End the practice of councils and the NHS purchasing homecare “by-the-minute”, alternatively focusing on achieving the outcomes people want.
- Support development of an expert-led workforce strategy for social care and a 10-year workforce plan, aligned with the NHS People Plan.
- Create a professional register for careworkers in England, covering all paid social care workers in both regulated and unregulated care services. Registration of careworkers needs to be adequately funded and carefully implemented.





